DIAGNOSIS
The clinical test follows these modes (first examination):
-
Short anamnestic investigation on previous scoliosis cases in family members and relatives (when necessary, recording the gathered information in a report)
-
chronological age
-
on the undressed subject (the woman wearing her panties and bra and the man wearing only his briefs), we note down the state and development of the secondary sexual characteristics, recording in the sheet whether the patient is prepubescent or pubescent:
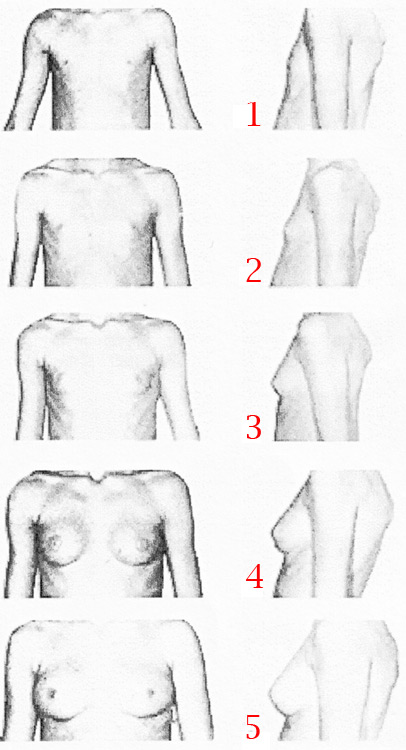
through the change in the tone of the voice and the presence of the first pubic hair in the boy and through the Tanner Test in the girl (fig. 6).
The patient must be evaluated standing straight and then with the trunk in forward flexion.
Standing position, frontally and posteriorly- the following must be found:
- a possible shift
- an asymmetry in the triangles of the built
- a projection in a shoulder blade
- an obliquity in the pelvis which must be rebalanced through lifts
In this phase of the examination, we look for possible “milk and coffee”, i.e. pale brown, spots on the skin which might a symptom of neurofibromatosic scoliosis or more seldom the presence of “pigmentation” areas and “tufts” of hair for congenital scoliosis or myelomeningocele.
Forward flexion of the trunk, bent on the waist by 80-90 degrees, with the feet alignd, the knees stretched out and the arms loose, we look the possible presence of the hump(s), noting down and recording the mm present in the measurements (forward or Adams’s bending) (fig. 7)
In order to carry out the measurement of the hump, we have recourse to a hump-meter (model by Dr. G. Felici or the like) (fig. 8) according to the following modes: we make the patient move from the standing position to the forward flexion position described above, until meeting with the eye the ideal dorsal plane upon which the hump is situated; so, choosing the point of greater difference in level between the two hemisomas, we apply the hump-meter (fig. 9): placing the level bubble horizontally, we evaluate the distance between the greater difference in level and the spinous apophysis of the rachis; said distance is reported on the contralateral hemisoma and in this point we measure in mm the distance existing between the instrument and the skin using a rule.
Lateral examination of the subject – standing straight and in lying position, on the examination couch – in order to detect a possible associated hyperkyphosis in the rachis (kyphoscoliosis) or, very seldom, an inversion in the kyphotic curve with a nearing of the rachis to the breastbone (lordoscoliosis).
With these data, recorded on the first check-up, we define the diagnosis as follows:
-
If no humps are found, we consider the scoliosis functional, not structured or false, not needing X-ray or any kind of therapy, except from examinations over time according to the patient’s age (fig. 10); we defuse the false disease informing the patient and his/her parents that the detected deformities (possible asymmetries, shifts, etc.) will disappear with time.
-
If, on the contrary, a hump is found (fig. 11), we measure and record it, suggesting clinical tests to be executed according to the period of growth; in case the measurement of the hump (or humps) shows a value lower than 7/8 mm, we do not recommend any R-ray analysis (see further on, table 2-3-4-5). We can therefore state with certainty that in the evaluation of a patient suffering from scoliosis we give the utmost importance to the presence of a hump, which characterizes structured scoliosis as a disease capable of progressing and getting worse: the hump does not disappear and can either remain unchanged – as it often happens – or change a little or even very much; that is why it is taken as a reference both for the prognosis and for the therapy against idiopathic scoliosis.
|
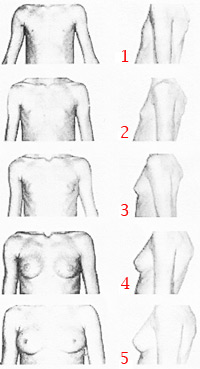
Fig. 6 – Tanner test
Phase 1 = a prepubescent patient
Phase 2 = widening of the areola
Phase 3 = further widening of the breast and of the areola
Phase 4 = further widening of the breast and of the areola
Phase 5 = an adult’s breast

Fig 7 – Forward bending Adams’ test = see description in the text
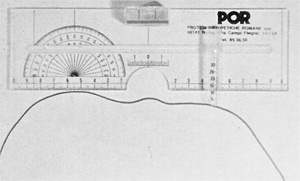
Fig 8 – Hump-meter by Dr Felici

Fig 9 See description in the text
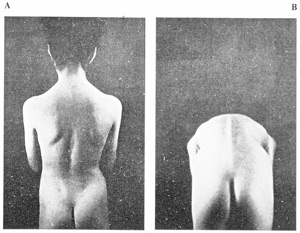
Fig 10 - Functional scoliosis or scoliotic attitude
In A = asymmetry in the triangles of the built, right shoulder blade higher than the contralateral one;
In B = forward flexion: absence of humpo
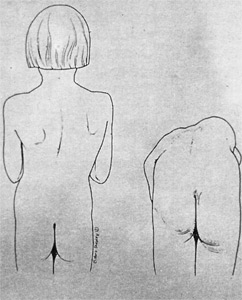
Fig. 11
|







{kind=link}